
Author: Billy-Joe Fryer / Editor: Charlotte Davies / Codes: / Published: 14/05/19
Medical gases are something used every day in the emergency setting, both pre-hospital and in-hospital, whether it be oxygen, medical air, or nitrous oxide. Each of these gases have their part to play in the emergency setting.
Cylinders:
We’re very used to using piped gases. Have you looked carefully at them? The oxygen inlet normally is all white, and then you plug the regulator in. The air inlet (if you’re allowed to use them) is black, and may have a guard on them. All of this is designed to stop us from accidentally connecting a patient to air instead of oxygen. The pins on the yoke that connect to the regulator are different. The piping is a different colour and each medical gas cylinder is a different colour, so you know at a glance what is inside.

It also has a different pin configuration, to make sure you can’t accidentally attach an entonox regulator to air – great! If you look at the hierachy of intervention effectiveness, then this is a perfect forcing mechanism.



The PIN system works on 7 holes, and the cylinder should match the regulator:
O2: 2 & 5
N2O: 3 & 5
Air: 1& 5
CO2: 1& 6
Heliox: 2& 4
This page or this site has more details on the PIN system. Here are two of the PINs we use in ED:
Oxygen – note the pin in 2 and 5
CO2 – note the pin in 1 and 6
The older molybdenum steel cylinders which are the A to J letters are charged to 137 bar gauge pressure. The newer ZA AS etc cylinders are Kevlar wound around aluminium and can tolerate much higher filling pressures. The letter indicates the cylinder size.
– A D size is charged to 2000psig (most references say lbs, but that’s technically not a unit of pressure, unless you’re being very lazy. I won’t argue with the PhD), 137 barg (bar is a measure of pressure difference. The g stands for gauge, and is important stuff to know…for engineers) and smaller cylinders charged more.
– They should be stored somewhere clean, dry, well ventilated, secure (safe from theft), and away from extremes of temperature. We have had our entonox stolen – I’m sure we’re not the only ones.
Lets break them down…
Nitrous Oxide

Nitrous Oxide, otherwise known as Entonox or “gas and air”, is a mixture of nitrous oxide (50%) and oxygen (50%). It is stored in similar (but different coloured!) cylinders to oxygen and can also be piped to wall sockets similar to oxygen outlets. Its use is simple and speedy and provides almost immediate analgesic effect to patients with moderate to severe levels of pain including labour pains. Its use however is contraindicated in patients with severe head injuries, agitation and patients at risk of decompression sickness (consider anyone that has been diving in the last 24 hours to be at risk). Caution should be used with suspected pneumothorax, bowel obstruction or polytrauma patients. It has minimal side effects and can be given for fast pain relief while different analgesia is prepared. As prolonged use can cause subacute degeneration of the spinal cord, we prefer not to use it in our patients with regular exacerbations of sickle cell disease – especially as, despite other claims, it seems to be addictive. BOC who make entonox have a very detailed guide here and free e-learning here. We know nitrous oxide works, but also that it makes you more susceptible to nocebo.
Nitrous Oxide is a drug of abuse and prolonged excessive exposure can cause complications such as spinal cord degeneration. Try to avoid using entonox for extended periods of time. It may be worth considering anticipatory management plans for frequent attenders within your department to ensure such risks are avoided.
There are some key things to remember when using nitrous oxide cylinders…
– Check the expiry date and turn the cylinder on ready for use.
– Remember microbial filters are single patient use
– The cylinder should be blue and the piping regulator should have a blue streak
– RCEM safe sedation guidelines suggest pulse oximitry monitoring
Oxygen

As I’m sure you’re more than aware, oxygen is one of the most commonly used drugs in emergency medicine and is utilised for a number of reasons including to improve oxygen availability in conditions such as COPD and asthma, anaesthesia, aiding resuscitation, major trauma, major haemorrhage and carbon monoxide poisoning.
Although used by clinicians probably on a daily basis, there’s more to using oxygen than just plugging the tubing to the supply and chasing the numbers around. In a 2018 National Patient Safety Alert, there were over 400 adverse incidents reported in the 3 years leading to 2018 regarding incorrect use of portable oxygen cylinders. As a result of this, 6 people died and many more were critically ill.
Using portable oxygen cylinders is common practice when transferring a patient between areas (e.g. resus to CT scanning or ED to ward), and is becoming more common in ambulance “offload corridors”. Here’s a few things to remember before you set off from the safety of piped oxygen:
– An oxygen cylinder is typically black with white shoulders, although new cylinders are white with O2 written all over them.
– Portable cylinders are not designed for prolonged use. When full, a standard ‘CD’ sized cylinder should operate for 30 minutes when used at a rate of 15LPM.
– Like every other drug, oxygen has an expiry date. Ensure your cylinder is not expired by observing the batch sticker located on the top of the cylinder.

– Remember to remove the tamper-evident hand-wheel cover (you can even recycle it and use it in wheelchairs and shopping trollies!).


- Follow the instructions on the black wheel to turn the cylinder on or off, and then set the flow rate using the separate flow dial normally found on the top of the cylinder.
When to take an ABG
The British Thoracic Society (BTS) (2017) recommend performing an ABG on the following patient groups:
– Any patient with hypercapnic risk factors who develops acute breathlessness, deteriorating oxygen saturation, drowsiness or any other features of carbon dioxide retention.
– Breathless patients who are thought to be at risk of metabolic conditions such at diabetic ketoacidosis or metabolic acidosis due to renal failure.
– Any other evidence in assessment or management that gives indication for blood gas analysis (i.e. unexpected change in NEWS or unexpected fall in oxygen saturation of 3% or more)
– Patients requiring increasing levels of inspired oxygen
You’ll know we’re moving away from arterial gases as a venous gas gives us all the information we need in the majority of circumstances. However, when we want to know someone’s oxygen pO2 and pCO2, a VBG just doesn’t cut it. Oh, and sats – remember the sigmoid curve.




Common Oxygen Delivery Devices
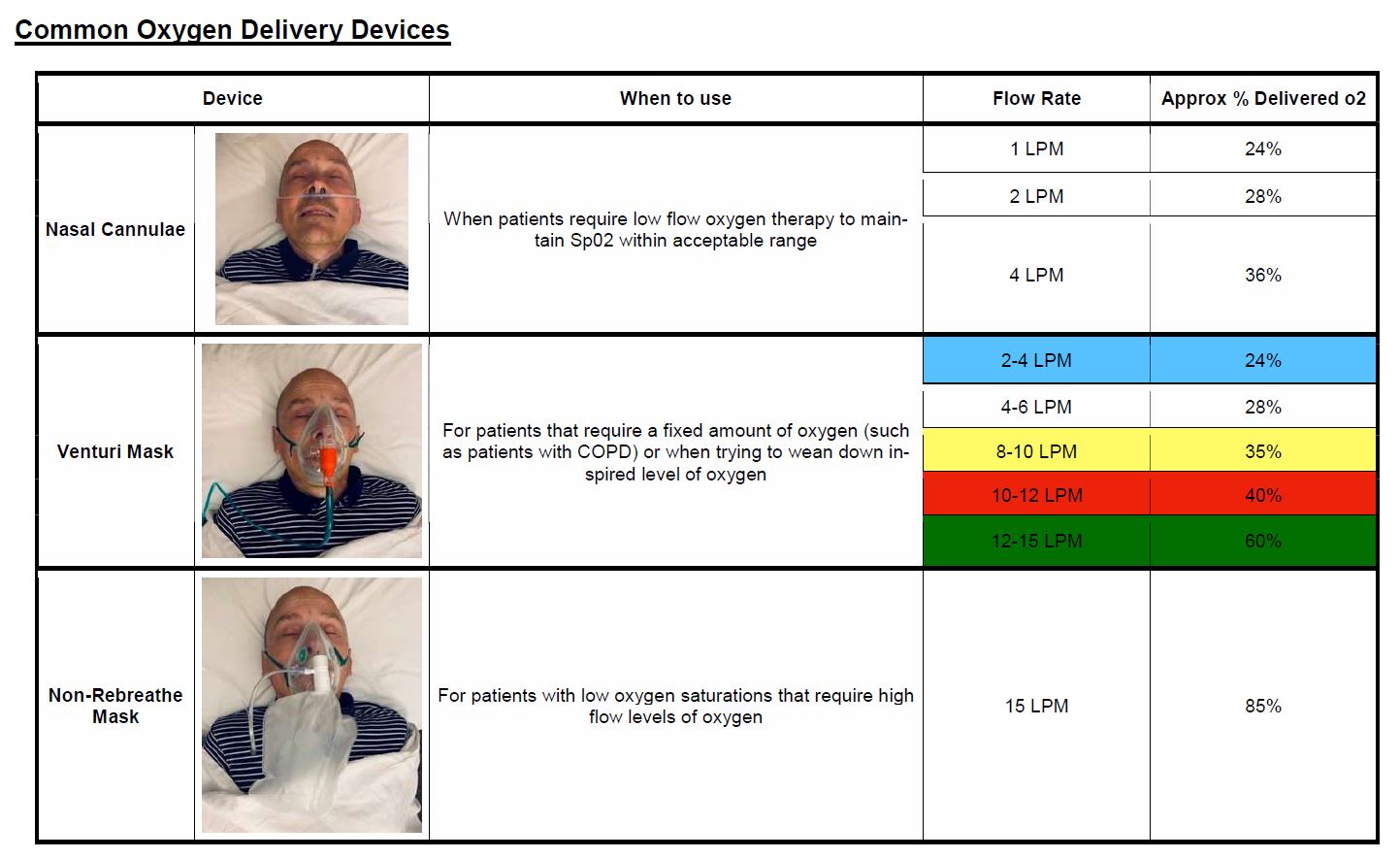
Based on the positive response to our Oxygen Delivery Devices poster last week, we’ve updated our #LightningLearning on the same topic + a bonus venturi device infographic! ?
EastMidsFOAMed (@EM3FOAMed) September 4, 2020
High-resolution printable PDFs available on our website ? https://t.co/cbhoW1hp5Y https://t.co/LYWmNgItBx pic.twitter.com/017xtoOh9H
There’s some fantastic one page summaries on oxygen delivery devices on onepageITU here – have a look at nasal specs,.
{kind=link}
There are also loads of awesome RCEMLearning resources that are free to look at and available to everyone. For this blog, we’d recommend reading about oxygen in human physiology, and listening about the hypercapnic drive.