Patent Ductus Arteriosus (PDA)
The ductus arteriosus connects the pulmonary artery to the descending aorta. In term infants, it normally closes shortly after birth and is completely closed in most infants by 2 to 3 weeks of age.
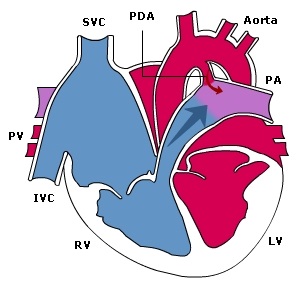
When there is a failure of ductal constriction after birth, the ductus arteriosus remains patent. The flow of blood across a PDA is then from the aorta to the pulmonary artery (i.e. left to right Fig 3), following the fall in pulmonary vascular resistance after birth. In the preterm infant, the presence of a PDA is not from congenital heart disease but due to prematurity (since muscularization of the medial layer occurs primarily in the third trimester).
Fig 3: Patent ductus arteriosus
Clinical presentation
| Symptoms |
|
| Physical signs |
|
Investigations
| Chest radiograph |
|
| ECG |
|
| Echocardiography |
|
Management
Surgical closure is the gold standard when indicated in the newborn period.
Indomethacin may be considered; it does, however, have the potential to cause necrotizing enterocolitis, intracranial hemorrhage, and renal toxicity.