CHD Lesions Presenting as Shock
-
Co-arctation of the aorta (severe)





Co-arctation is not always severe. Lesions are defined as critical when the systemic circulation depends on ductus arteriosus patency. It can also remain asymptomatic until adulthood. It is often associated with other abnormalities such as a VSD or bicuspid aortic valve.
Examination/investigation findings
- Examination:
- Absent femoral pulses or Radio-femoral delay before the DA closes,
- Cyanosis
- 4 limb BP discrepancies – gradient of >10mmHg between upper and lower limbs is clinically significant
- Signs of CCF
- Investigation
- Diagnosis is usually made antenatally via USS scan
- ECG may show LVH or RV conduction delay
- CXR: may show figure of 3 sign (see below)
- All patients should have either cardiac MRI or CT for evaluation of thoracic aorta prior to definitive management

Management
- Rapid A-E assessment of collapsed neonate
- Prostaglandin infusion if duct-dependent circulation
- Diuretics to reduce preload combined with volume replacement to correct metabolic acidosis
- Surgery usually performed within 24 hours removal of the narrow segment
-
Hypoplastic left heart syndrome




This is a common diagnosis with around 260 cases in the UK annually (Barron et al, 2009). It is usually diagnosed prenatally. Initially, most patients with HLHS will be haemodynamically stable. Over several days, as pulmonary vascular resistance falls and the DA closes, the ratio of pulmonary to systemic blood flow will increase. This causes increased rightleft shunting which leads to cyanosis, congestive heart failure, shock and respiratory distress.
Examination/Investigation findings
- Examination:
- Absent femoral and brachial pulses, delayed CRT, hypotension secondary to shock
- Signs of right heart failure enlarged liver, tachypnoea, rales
- Shock and respiratory distress secondary to acidosis upon DA closure
- May have PDA murmur (see section on PDA)
- Investigations
- ECG: absent LV forces
- CXR: cardiomegaly
- Echo is gold standard for diagnosis
Management
- Patients should be born in a cardiac centre
- Prostaglandin infusion to maintain DA patency
- Surgery within 3-5 days surgical management is staged and requires 3 operations to establish a single ventricle circulation (Hosein et al, 2007)
- Norwood Procedure neonatal period creation of common atrium by removal of atrial septum, Pulmonary arteries attached to a reconstructed aortic arch to create a single outlet right sided heart. Pulmonary circulation provided by BT shunt (shown) or an RV to PA conduit.

- Glenn 4-6 months SVC connected to pulmonary arteries. Venous return from the head and neck is routed directly to the lungs which allow saturations to reach 80-85%. The BT shunt/conduit is removed. By 3-5 years, there will be insufficient blood returning from the head and neck to keep the child well so a Fontan is required.

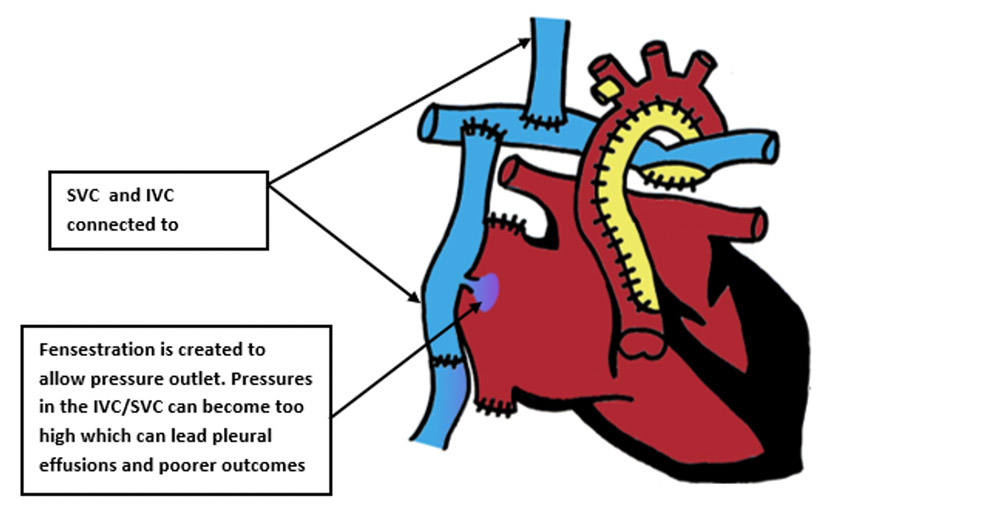
3. Fontan 3-5 years IVC connected to the pulmonary circulation so venous return from the body is routed directly to the lungs which allows saturations to reach 90-95%. Most patients with a Fontan circulation reach adulthood but must undergo long term follow up. Many are able to manage school/jobs and some female patients are even able to undergo pregnancy and delivery!
Learning bite
The most common CHD lesions that can present as shock are severe co-arctation of the aorta and hypoplastic left heart syndrome. Both require surgical correction.