Paediatric Triage
Children and infants are commonly involved alongside adults in disasters or MCIs (10). Triaging of paediatric patients is challenging; due to the different normal physiological values for paediatric patients, the triage algorithms described previously are not appropriate, and different tools must be remembered. Paediatric triage is also emotionally challenging, and even when using the appropriate tools discussed below, there is a tendency for healthcare personnel to overtriage children at the expense of more unwell adults.
Paediatric Triage Tape
A simple way to combat some of the challenges of triaging paediatric casualties is with the use of paediatric triage tape. This can be used to measure the casualty’s length from heel to top of head, and the estimated weight as well as a triage sieve algorithm with suitably adjusted values, can be read off the tape at the appropriate point.

Fig 5: Use of paediatric triage tape
JumpSTART algorithm
If a paediatric triage tape is not available, clinicians can substitute age-adjusted physiological variables in the adult triage sieve tool themselves. This does, however, depend on the clinician being able to accurately estimate the patients weight, and also remember the normal values for heart and respiratory rate for a number of different age brackets. A perhaps simpler alternative is the JumpSTART Pediatric MCI Triage Tool (11) and this is advocated within the 2018 NHS England Clinical Guidelines for Major Incidents. This avoids the need for weight calculations or estimations and may be used for any patient who ‘appears to be a child’. The JumpSTART algorithm is as follows:
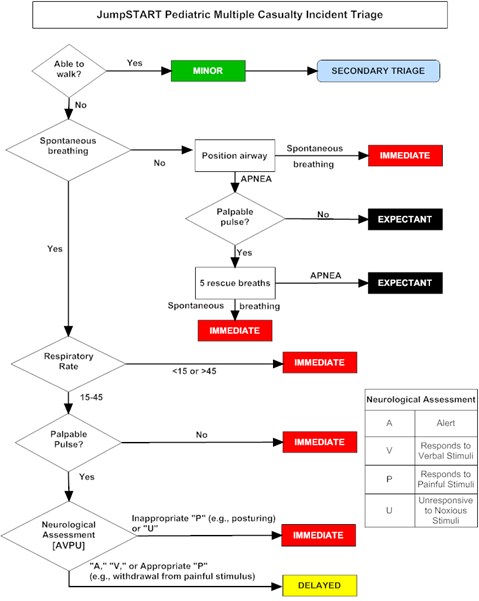
JumpSTART paediatric triage algorithm (11)
It is clear from this flowchart that the JumpSTART algorithm considers similar physiological parameters to the MPTT24 adult triage tool discussed above, however to account for the variability of normal physiological values in paediatric patients, a broader normal range for respiratory rate is used, and simply the presence or absence of a pulse as the cardiovascular measure. Studies have shown this tool to be easily remembered by clinicians and to improve accuracy of triaging paediatric patients (12).
However, the evidence to support any of the existing paediatric major incident triage tools is limited, with both the Paediatric Triage Tape and the JumpSTART method having poor sensitivity at identifying children in need of life-saving interventions (42% and 1% respectively) (13). Work is currently ongoing within the UK to try and identify a bespoke paediatric primary major incident tool that demonstrates improved performance at identifying those children who need life-saving interventions.