
Author: Gavin Lloyd / Editor: Jason M Kendall, Stewart McMorran / Reviewer: Thomas MacMahon, Kathryn Blackmore / Codes: T1 / Published: 30/08/2023
For each life-threatening thoracic injury this work will include:
- A definition and context to include the incidence, likely mechanism of injury and (where appropriate) the likelihood of the injury being missed clinically and/or radiologically
- Clinical assessment and identification of the injury
- Treatment
- Key learning points, pearls and pitfalls
Definition and Context
This is an expanding pneumothorax that increasingly limits ventilation and venous return. It is not an on/off phenomenon, rather a continuum.
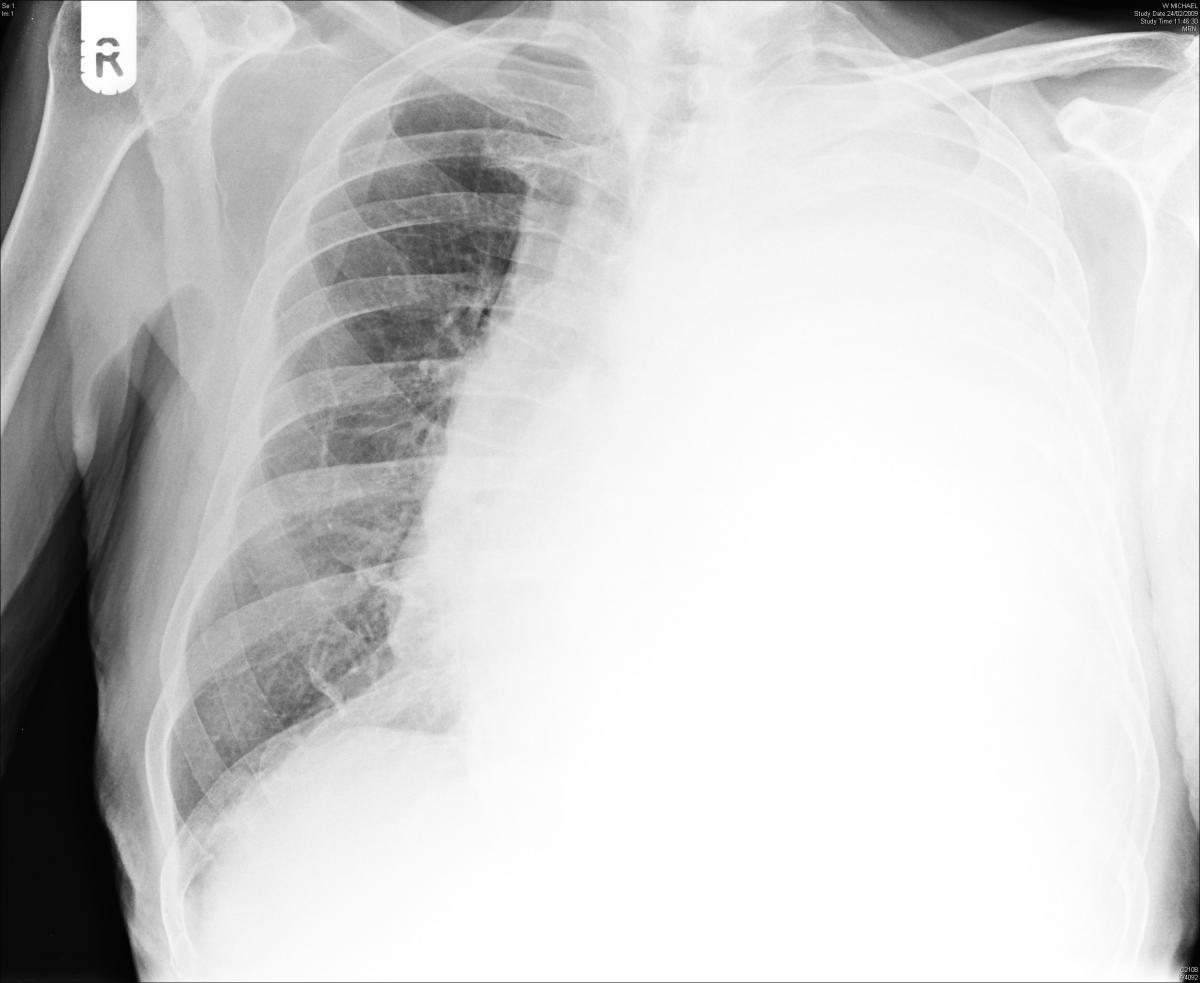
So even impressive expansion (see image), may be well tolerated in young individuals with no comorbidities and no other injuries. In fact it may be tolerated so well that you may miss the clinical diagnosis.
Fig 1: Tension pneumothorax

Given that the expansion is dynamic, be vigilant in patients with a chest x-ray proven small pneumothorax in whom you elect not to insert a chest drain.
Clinical Assessment and Identification
Symptoms and signs depend on where your patient is on the expanding pneumothorax continuum clinical features become more obvious with expansion.
(a) For awake patients:
Universal features of tension pneumothorax are chest pain and respiratory compromise [1], neither of which are discriminatory of course.
Low oxygen saturations may be an early feature; hypotension tends to be late. Both may have other causes.
Lateralising the pneumothorax may not be straight forward. Listen for decreased breath sounds on the affected side, and it may be better to listen in the axillae rather than over the anterior chest wall.
Note the classical signs of hyper-resonance and tracheal deviation are soft.
Bedside chest ultrasound is being increasingly used in the diagnosis of pneumothorax and has a high sensitivity
(b) For ventilated patients:
Early reliable signs are:
- Decrease in oxygen saturations this is likely to be prompt
- Decrease in BP
- Tachycardia
Look too for raised ventilation pressure (greater than 40) ensure that the ventilator pressure alarm settings are set appropriately (Fig 2). Lateralising signs are the same as for awake patients.
Fig 2: Ventilator

If your patient is not critical (we have not defined that; use common sense), then you may have time to perform an urgent bedside thoracic ultrasound scan (USS). However, this should not delay emergent treatment in a deteriorating patient. This should help you:
- Confirm or refute the diagnosis
- Confirm the side of pneumothorax
- Rule in or out other diagnoses
Learning Bite
X-ray imaging is not recommended for the diagnosis of a tension pneumothorax if there are suspicions, proceed with decompression and image afterwards.
Treatment
Needle thoracocentesis or finger thoracostomy is advocated for tension pneumothorax in the first instance as per ATLS. This then needs to be followed by a chest drain [2].
The recommended site for needle thoracocentesis in adults is now the 5th intercostal space, just anterior to the mid-axillary line. In children, it is still the 2nd intercostal space in the mid-clavicular line. The site for finger thoracostomy in both is still the 5th intercostal space, just anterior to the mid-axillary line.
Potential drawbacks to this strategy are:
- You might deem a lack of hiss (or bubbling, if you have put some saline in a syringe attached to the needle) as evidence of no tension pneumothorax the procedure doesnt have 100% specificity.
- A (4.5 cm) 14 gauge cannula may not reach the pleural space via the second intercostal space. In one study [3], this was the case in about a third of the patients This might account for the point above
- The cannula can kink and cease to function and it should not be taped down to secure, as this kinks it
- You may cause a pneumothorax if the diagnosis is incorrect. This is of particular concern if the patient receives IPPV but this shouldnt prevent you from proceeding to decompress if suspicion is high.
In peri-arrest patients with suspected tension pneumothorax (particularly those with penetrating trauma) a thoracostomy (i.e. the initial part of a chest drain insertion) is probably the best option.
Learning Bite
Avoid needle thoracocentesis in peri-arrest patients with suspected tension pneumothorax – thoracostomy is the better option.
Chest Drain Insertion
Chest drain insertion is covered in detail in a dedicated skills session here.
Here are some selected key learning points from that session:
- The most common cause of serious injury (and death) as a result of chest drain insertion, is insertion at the incorrect site, usually too low
- Confirm that the drain lies within the chest wall cavity by looking for fogging of the tube and swinging of the chest drain with respiration
- Do not clamp the chest drain or apply suction unless otherwise advised by Cardiothoracics
- The underwater seal needs to remain below the insertion site at all times
Pearls
- If you do perform needle thoracocentesis, have some saline in the syringe to demonstrate bubbling when the tension is hit
- Gross surgical emphysema in combination with pneumomediastinum (as per chest X-ray (CXR)) and a chest drain that continues to bubble, suggests tracheo-bronchial injury (Fig 3)
- If there is good clinical and radiological evidence of significant lateral chest wall injury, consider the second intercostal space anteriorly for the chest drain insertion its safer for the operator and less painful for the awake patient.
Fig 3: Tracheo-bronchial injury

Pitfalls
- One third of initial CXRs in trauma will not detect pneumothorax. Anaesthetic colleagues need to be aware of this if your patient leaves for theatre.
- Cardiac tamponade may give similar signs clinically shock, with distended neck veins. A combination of your eFAST skills and consideration of the mechanism of injury should help you distinguish the two
- Beware other pathology masquerading as large (possibly tensioning?) pneumothorax on the CXR, for example an emphysematous bulla or gastrothorax (Figs 4 and 5). Reconsider the clinical presentation and consider CT where the CXR diagnosis remains in doubt
Fig 4: Emphysematous bulla

Fig 5: Gastrothorax

Definition and Context
For an open pneumothorax, think hole in the chest. It is also known as a communicating pneumothorax or sucking chest wound.
Rare – typically caused by ballistic (shot gun) injury, and clearly unlikely to be missed clinically.
As the patient takes a breath in, the hole in the chest competes with the normal airway (mouth/nose to trachea) for delivery of air.
Learning Bite
A hole of only 1 or 2 cm in diameter may cause serious respiratory compromise, particularly in patients with comorbidities, and/or other injuries.
Clinical Assessment and Identification
Prompt clinical inspection front and back; a small sucking chest wound is usually audible.
Treatment
Definitive treatment is surgical repair. The emergency physician must alleviate any respiratory embarrassment, exclude associated injuries and identify the need for timely thoracotomy or laparotomy.
- Cover the wound taping down three sides only, in order to allow expired air to escape, if not already done so by the paramedics. Sheets of Jelonet or any other impermeable membrane will do. Specific chest seal devices (Ashermann or Bolin) exist (Fig 6).
- If the hole is too big for either of the above, then cover with a large opsite, make a small hole in the middle and place a chest seal device on top if available
Fig 6: Chest seal devices

- Any dressing over the wound should not be occluded on all four sides to allow for a flutter valve effect. Temporarily release any wound dressing over the open pneumothorax if you suspect tensioning is starting to occur.
- Early intubation: IPPV solves the respiratory embarrassment created by the hole in the chest
- For small open pneumothoraces, insert a chest drain remote from the wound on that side; this is practically easier once the patient is anaesthetised
- Do not insert a chest drain in patients with a large open pneumothorax since muscle flaps may be needed for closure and can be damaged in the procedure.
Definition and Context
A massive haemothorax is a haemothorax >1500 ml, or one-third of the patient’s blood volume according to ATLS. It is uncommon, can be blunt or penetratingusually penetratingand unlikely to be missed, radiologically.
It creates a problem because of shock (haemorrhagic and impaired venous return from the vena cava) and decreased ventilation (the lung on that side gets compressed).
Clinical Assessment and Identification
A massive haemothorax is an expanding haemothorax. The signs will be less reliable in diagnosing a moderate haemothorax.
Listen at the lung bases (Fig 7). There should be clear signs of shock prompting you to consider the diagnosis. Use CXR and eFAST to guide you.
Fig 7: Lung bases
FAST signs: the absence of a mirror image of liver/ lung or spleen/lung across the diaphragm suggests a haemothorax (Fig 8); alternatively free fluid in the abdomen alone should prompt you to reconsider the source of haemorrhage (Fig 9).
Fig 8: Haemothorax
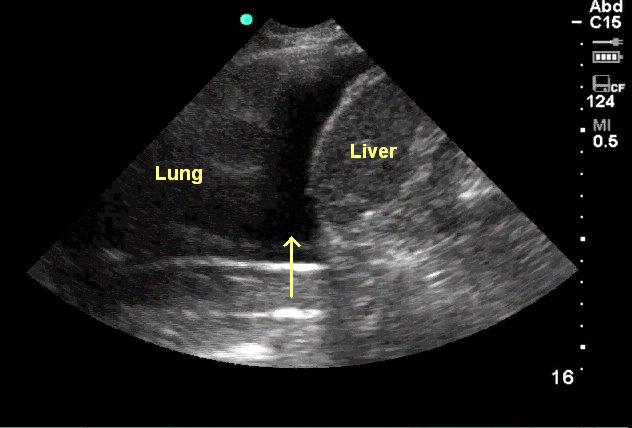
Fig 9: Free fluid

Treatment
Treatment is focused on simultaneously 1) restoring blood volume while also 2) decompressing the chest.
- Use blood and blood products early, with activation of your major haemorrhage protocol if necessary and never insert a chest drain without first ensuring that there is IV access and blood products to hand.
- Uncrossmatched blood may be needed and is infinitely preferable to crystalloid in this setting (current ATLS guidelines suggest using no more than 1L of crystalloid before as a temporising measure until blood is available).
- A 28-32F chest tube should be placed to decompress the chest and improve ventilation.
- Ideally, connect the drain to a cell salvage/saver machine (autotransfusion) (Fig 10). If a cell saver is not readily available, use the usual apparatus, but prime the underwater seal with saline sterile water. The saline/blood collection can still be run through a cell saver later.
Fig 10: Cell salvage/saver machine

- >1500ml of blood immediately returning from the chest tube is generally an indication for an urgent thoracotomy. Involve your cardiothoracic surgeons early in the care of these patients.
- Occasionally a massive haemothorax may be well tolerated, typically in young patients with a chest stabbing. Delaying chest drain insertion until reaching thoracic theatre, where cell salvage exists, is an option depending on availability of skills and theatre space.
| ATLS indications for thoracotomy [2] |
|
Pitfall
You may underestimate the size of the haemothorax on a supine CXR (Fig 11). Use eFAST in preference during your initial assessment.
Fig 11: Haemothorax

Learning Bite
- In massive haemothorax, equal attention should be paid to restoring blood volume and decompressing the chest.
- Involve your cardiothoracic surgeons early in the care of these patients.
- Prime the underwater seal for the chest drain with saline not sterile water.
Definition and Context
Cardiac tamponade is a collection of fluid (blood in the context of trauma) in the pericardial sac causing haemodynamic compromise.
When faced with a penetrating injury to chest, back or upper abdomen, think tension pneumothorax, think massive haemothorax, and think cardiac tamponade. Exclude or confirm tamponade with a eFAST scan.
Cardiac tamponade is not an on/off phenomenon (yet another continuum), though the progression to PEA cardiac arrest may be rapid. 50 to 200 ml of blood in the pericardial sac may be enough to cause this.
Cardiac tamponade as a result of blunt injury is exceptionally rare in those patients reaching hospital alive.
Clinical Assessment and Identification
eFAST has particularly high sensitivity about 95% according to ATLS [2].
Do note that there are drawbacks in detecting and interpreting the classical clinical signs:
- Neck veins may not be distended if the patient has haemorrhagic shock
- Hypotension (and a raised respiratory rate) may have other causes
- Muffled heart sounds unlikely to be heard in the ED!
Treatment
- Fluid resuscitation to increase pre-load
- If the patient is haemodynamically stable refer for urgent surgical exploration in theatre. Look for co-existing injuries (especially pneumothorax) on a portable CXR first
- Thoracotomy if the patient presents within 10 minutes of cardiac arrest
- Correctly performed pericardiocentesis is likely to fail because the blood within the pericardium is clotted. The procedure will also delay thoracotomy. We (the authors) advise against pericardiocentesis unless there is really no one capable of opening the chest. ATLS [2] advises pericardiocentesis only as a temporising measure, pending thoracotomy
Learning Bite
- Cardiac tamponade as a result of blunt injury is exceptionally rare
- eFAST scanning is highly sensitive
- Thoracotomy, not pericardiocentesis, is recommended
Definition and Context
This occurs when a series of ribs (usually 3 or more) are fractured segmentally (i.e. in more than one place) resulting in a free or floating section of the chest wall. This injury is relatively common small flails may be missed clinically.
Learning Bite
- Beware underlying pulmonary contusions which are inevitable, and may cause significant morbidity and mortality in any age group.
- Considerable force is required to create a flail chest in young people. Look carefully for other injuries, both intra and extra-thoracic.
- Multiple rib fractures are a potential source of significant haemorrhage
Clinical Assessment and Identification
Fig 12. A 3D reconstruction from a CT scan showing a flail chest via Wikimedia

Identification is by palpation as well as inspection.
A CXR might identify associated pneumothorax, haemothorax and pulmonary contusions (Fig 12). The appearance of early pulmonary contusions is particularly worrying, and evidence of further and perhaps more extensive contusions with physiological effect may evolve.
Fig 13: Pulmonary contusions
Treatment
Your treatment options depend largely on the respiratory embarrassment caused consider:
- Your patients clinical condition
- The size of the flail chest
- Associated injuries
- Age
- Co-morbidities
- Destination from resus (theatre, CT scan, ITU or ward)
For patients with major trauma (apply common sense in defining this), proceed to intubation and ventilation intermittent positive pressure ventilation (IPPV).
- Take better control of respiratory compromise
- Address your patients pain (remember to give adequate analgesia post rapid sequence induction (RSI))
- Facilitate clinical procedures e.g. chest drain insertion and CT scan
Insert a chest drain for associated pneumothorax and haemothorax. CT is likely to pick up occult pneumothoraces.
Judicious fluid resuscitation since excessive fluid floods injured lung tissue.
Definitive surgery (internal fixation of ribs) at the discretion of cardiothoracic surgeons.
Discuss treatment options with ICU and thoracic surgical colleagues for patients with a flail segment causing limited respiratory embarrassment, and in whom there are no other life-threatening injuries. A conservative approach might include the use of thoracic epidural [4], intercostal nerve blocks or patient controlled analgesia, and continuous positive airway pressure (CPAP) and physiotherapy.
Definition and Context
Bruised lung; unlikely to be missed radiologically unless the CXR is early.
Potentially life threatening since:
- The patient is at risk of hypoxaemia
- Because of the force involved to cause the injury, associated injuries are common
- Injured lung is vulnerable to flooding from aggressive fluid resuscitation
Patients with co-morbidities and/or advanced age are particularly at risk from this injury.
Clinical Assessment and Identification
Look for patchy white areas progressing to frank consolidation on the CXRaspiration and haemorrhage are differential diagnoses. (Fig 13)
Fig 14: Lung contusion

Contusions visible on the initial CXR suggest significant injury, with further radiological changes and blood gas derangement likely to follow.
Look for associated rib fractures and haemo/pneumothorax.
Rib fractures do not always co-exist, particularly in the young, where their existence indicates that significant force created the injury.
Treatment
Consider the following:
- IPPV and positive end-expiratory pressure (PEEP) for the sicker patients
- Judicious use of fluids consider insertion of a central line and arterial line
- No evidence for steroids or prophylactic antibiotics
- Avoid colloids since these will breach injured lung tissue and worsen hypoxia
- Discuss disposal of each patient with ITU and thoracic surgical colleagues
- Lung contusion is a marker of significant injury
- Early CXR evidence of contusion is particularly worrying
- Oxygen therapy to keep saturations within target range
Definition and Context
Myocardial bruising caused by blunt injury, including deceleration and ballistic mechanisms.
The key problem with interpreting the literature is the lack of a diagnostic gold standard (apart from post mortem).
Clinical Assessment and Identification
- Unexplained tachycardia may be a clue. Also look for atrial and ventricular ectopics.
- Consider bedside echocardiogram.
- Consider use of troponin for evidence of myocardial injury [5]
- Persistent hypotension with no clear haemorrhage is also suspicious for myocardial injury (once spinal and obstructive causes are ruled out).
Treatment
There is no direct ED-based intervention to treat the myocardial contusion itself; treat the following if identified [6]:
- Fluid resuscitation with CVC monitoring to guide fluid management
- Cardiac monitoring, as arrhythmias are common in myocardial injury
- Arterial line and blood gas monitoring to ensure hypoxaemia or disturbances in acid-base balance are addressed, as these can also precipitate arrhythmias.
- Treat any arrhythmias expectantly as per ALS guidelines
- Early ECHO
Pitfall
Beware labelling ST changes as myocardial contusion; there may have been a primary cardiac event that precipitated the accident.
Definition and Context
Consider carefully in rapid deceleration injuries, e.g. road traffic accidents and falls. Missing the diagnosis both clinically and on CXR is quite common.
The few patients (about 10%) who make it alive to the ED will have haemorrhage tamponaded by aortic adventitia (a vulnerable pseudo-aneurysm).
There is no increased risk of injury related to atherosclerosis. It is young males who engage most in risk taking activities that end in rapid deceleration accidents (Fig 14).
Fig 15: Rapid deceleration accident

Clinical Assessment and Identification
Most patients will complain of other associated injuries rather than specific symptoms of aortic injury.
The majority of ruptures in patients reaching hospital alive are just distal of the left subclavian artery, so a difference in blood pressure between both arms is not necessarily a feature.
Occasional clinical clues include generalised hypertension, upper extremity hypertension in combination with weak or absent femoral pulses, and a harsh systolic murmur.
An erect good-quality CXR has good but not perfect sensitivity in ruling out the diagnosis in low risk patients [7]. Such a CXR is not achievable in most multi-trauma patients, Neither are these patients necessarily low risk. Several CXR features might suggest the injury according to ATLS [2].
Several CXR features might suggest the injury according to ATLS [2]:
- Widened mediastinum the most reliable sign
- Fractures of the first and second ribs
- Obliteration of the aortic knob
- Deviation of the trachea to the right
- Presence of a pleural cap
- Elevation and rightward shift of the right main stem bronchus
- Depression of the left main stem bronchus
- Obliteration of the space between the pulmonary artery and the aorta
- Deviation of the nasogastric tube to the right
Contrast CT thorax is the investigation of choice.
Aortic injury is one of many causes of mediastinal haematoma; sternal fracture and thoracic vertebral fracture are also associated with mediastinal haematomas (Fig 15).
Fig 16: Mediastinal haematoma

Treatment
Surgical repair or endovascular stenting, which may require transfer from your facility. Competing and likely overriding injuries include life-threatening head, abdominal or pelvic injuries.
Control hypertension (systolic no more than 110 mmHg) and tachycardia with appropriate analgesia; labetalol is the agent of choice to control acute hypertension in this setting.
Learning Bite
Young males are the most likely candidates for aortic injury
Definition and Context
Diaphragmatic injury is usually caused by penetrating rather than blunt injury. It is easily missed both clinically and radiologically.
In blunt injury it is three times more common on the left (the right hemi-diaphragm being protected by the liver) and nearly always at the weakest point, posterolaterally.
A diaphragmatic breach will not heal spontaneously because of the differential pressure gradients between chest and abdomen. Abdominal content herniation is a possibility and may be picked up years later.
Figs 17 and 18: Diaphragmatic injury


Clinical Assessment and Identification
Symptoms are likely to be masked by associated injuries.
Diaphragm injuries resulting from knives or bullets are more likely to be detected on surgical exploration.
In blunt injuries, particularly those causing an abrupt rise in intra-abdominal pressure, be careful not to interpret a gastrothorax (Fig 18) for a large pneumothorax; both will cause respiratory embarrassment.
Fig 19: Large gastrothorax

Treatment
Consider the following:
- Insert a nasogastric tube gently to drain stomach content. The insertion of the chest drain is to drain any associated pneumo/haemothoraces.
- A cautiously placed chest drain using the traditional open technique, not Seldinger, is indicated
- Surgical repair needs to be considered in the context of associated injuries
- Examine the CT carefully in patients who have sustained a (blunt) abrupt increase in intra-abdominal pressure
- Diaphragmatic injury needs excluding by your surgical colleagues in cases of penetrating injury requiring theatre.
Oesophageal injury
This rare injury is often initially missed both clinically and radiologically.
Other associated injuries will normally predominate the clinical presentation e.g. a neck stabbing with tracheal and vascular disruption.
Operative repair or endoluminal stenting should be considered in the context of other associated injuries.
Definition and Context
This rare injury is typically caused by significant deceleration injuries; most patients die at the scene of the accident. It is unlikely to be missed clinically or radiologically in survivors, since clinical effects are usually dramatic.
Clinical Assessment and Identification
Fig 20: Tracheo-bronchial injury

A massive air leak is suggested by gross surgical emphysema, pneumomediastinum and a vigorously bubbling chest drain that has failed to alleviate respiratory compromise. (Click the image to see a larger version).
Haemoptysis is an additional clue.
Treatment
Discuss intubation strategy with senior anaesthetic colleagues (consider single or double cuffed tubes, use of fibre optics, etc).
Consider additional large bore chest drain on the affected side (one intercostal space further up). Do not attach suction to the chest drain.
Other significant patient injuries may influence your resuscitation strategy.
Learning Bite
Two large bore chest drains may be needed to counter the air leak of a tracheo-bronchial injury.
Simple Pneumothorax
This is a common injury which is readily missed on CXR and subsequently discovered on CT.
Small, asymptomatic/occult pneumothoraces may be observed, even if the patient is ventilated [8]. About a third may deteriorate clinically, necessitating a drain.
No guideline regarding the safe timing for flying following a simple traumatic pneumothorax exists. A pragmatic approach may be to adopt British Thoracic Society guidelines for spontaneous pneumothorax: flying is permissible, once chest x-ray confirms resolution of the pneumothorax.
Fig 21: Simple pneumothorax

Haemothorax
Fig 22: Haemothorax on a supine

Common, typically caused by intercostal vessel injury (high arterial pressure system, and, therefore, potentially brisk bleeding) or more rarely, lung laceration (low arterial pressure system).
Two errors in CXR interpretation:
- Failing to recognize haemothorax on a supine CXR (image)
- Underestimating the size of haemothorax. Blunting of a costophrenic angle on an erect CXR requires at least 300 ml of blood
Treatment
If a haemothorax is large enough to be visible on CXR, then insert a large bore chest drain (28-32F) using the traditional surgical technique in order to [8]:
- Evacuate the blood, so preventing a clotted haemothorax (and consequent lung entrapment +/- empyema)
- Monitor blood loss
Give prophylactic antibiotics as guided by your local antibiotic prescribing policy.
Enrol the support of thoracic surgical colleagues for >moderate haemothorax. ATLS [2] recommends thoracotomy for:
- Prompt drainage of 1500 ml blood
- >200 ml/hr blood loss for 2-4 hrs
- Continued need for blood transfusion
Do not forget that empyema rates following chest drain insertion for any traumatic indication is approximately 2.5% – give your patients prophylactic antibiotics (cephalosporins or clindamycin) [9].
Learning bite
A haemothorax visible on chest x-ray requires a large bore chest drain.
Rib Fractures
Significant force is required to break ribs in the young; underlying injury is typical, especially lung contusions. Whilst less force is required in the elderly, even an isolated rib fracture can result in significant morbidity (e.g. secondary pneumonia) particularly in those with pre-existing comorbidities.
In addition to standard therapy consider the role of patient-controlled analgesia, thoracic epidural and physiotherapy for vulnerable patients.
Sternal Fractures
These are relatively benign injuries but may be associated with underlying myocardial or pulmonary contusion. Depending on the mechanism, screen also for any associated neck injury given the forces involved. Consider the role of patient-controlled analgesia or local anaesthetic via a sternal catheter [10] in vulnerable patients.
Fig 23: Sternal fracture

Posterior Sternoclavicular Joint Dislocation
This an exceptionally rare injury. It is clinically important since the medial clavicular head may compromise the airway or major vessels.
If there is evidence of compromise, reduction of the dislocation should be attempted. Abduct the arm to 90 and extend 10-15 and apply traction (with counter attraction to the torso from another colleague); maintain traction and pull the medial end of the clavicle forward with your fingers and thumb. If this fails, prepare the skin with iodine and local anaesthetic and repeat with a towel clip [10].
- eFAST is recommended as a rapid assessment for tension pneumothorax, unless the patient is critically ill. A portable CXR may also help. Radiological evidence of tensioning does not necessarily correlate clinically
- Avoid needle thoracocentesis in peri-arrest patients with suspected tension pneumothorax thoracostomy is the better option.
- The most common cause of serious injury (and death) as a result of chest drain insertion, is insertion at the incorrect site, usually too low
- Confirm that the drain lies within the chest wall cavity by looking for a fogging of the tube and swinging of the chest drain on respiration
- A hole of only 1 or 2cm in radius may cause serious respiratory compromise, particularly in patients with comorbidities, and/or other injuries
- Prime the underwater seal for the chest drain with saline not sterile water for suspected massive haemothorax
- Cardiac tamponade as a result of blunt injury is exceptionally rare
- eFAST is highly sensitive in detecting blood in the pericardium
- Thoracotomy, not pericardiocentesis is recommended for cardiac tamponade
- Pulmonary contusions are near inevitable in patients with a flail chest, and may cause significant morbidity and mortality in any age group
- Lung contusion is a marker of significant injury
- Early CXR evidence of pulmonary contusion is particularly worrying
- Multiple rib fractures are a potential source of significant haemorrhage
- A haemothorax visible on chest x-ray requires a large bore chest drain
- A normal ECG effectively rules out myocardial contusion
- Young males are the most likely candidates for aortic injury
- Examine the CT carefully in patients who have sustained an abrupt increase in intra-abdominal pressure
- Diaphragmatic injury needs excluding by your surgical colleagues in cases of penetrating injury requiring theatre
- Two large bore chest drains may be needed to counter the air leak of a tracheo-bronchial injury.
- Leigh-Smith S, Harris T. Tension pneumothoraxtime for a re-think? Emergency Medicine Journal 2005;22:8-16.
- ATLS Subcommittee; American College of Surgeons Committee on Trauma; International ATLS working group. Advanced trauma life support (ATLS ): the ninth edition. J Trauma Acute Care Surg. 2013 May;74(5):1363-6.
- Wax DB, Leibowitz AB. Radiologic assessment of potential sites for needle decompression of a tension pneumothorax. Anesth Analg. 2007 Nov;105(5):1385-8, table of contents.
- GA McLeod, FRCA , C Cumming, FRCA, Thoracic epidural anaesthesia and analgesia, Continuing Education in Anaesthesia Critical Care & Pain, Volume 4, Issue 1, February 2004, Pages 1619.
- Jackson L. Use of troponin for the diagnosis of myocardial contusion after blunt chest trauma. Best Bets, 2005.
- Kaye P, OSullivan . Myocardial contusion: emergency investigation and diagnosis. Emergency Medicine Journal 2002;19:8-10.
- Ekeh AP, Peterson W, Woods RJ, et al. Is chest x-ray an adequate screening tool for the diagnosis of blunt thoracic aortic injury? J Trauma. 2008 Nov;65(5):1088-92
- Henry S. ATLS 10th edition offers new insights into managing trauma patients. Bulletin of the American College of Surgeons, 2018.
- Butler J. Antibiotics in patients with isolated chest trauma requiring chest drains.Best Bets, 2002.
- Macdonald PB, Lapointe P. Acromioclavicular and sternoclavicular joint injuries. Orthop Clin North Am. 2008 Oct;39(4):535-45, viii.
- Jenner R. Chest drains in traumatic occult pneumothorax. Best Bets, 2006.
- Appelboam A, McLauchlan CA, Murdoch J, MacIntyre PA. Delivery of local anaesthetic via a sternal catheter to reduce the pain caused by sternal fractures: first case series using the new technique. Emerg Med J. 2006 Oct;23(10):791-3.